




Maybe COVID-19 isn’t that dangerous? (and the country should mostly ignore it)
JP Sears is an irreverent comedian. He made a video poking holes in the mainstream story of COVID-19. He claims:
1. You should do what you think is best based on your own assessment and accept the consequences of your decision.
2. Original estimate of death rate of 4.5%. LA County study shows incidence is 25X-40X higher, so the actual death rate is lower. New estimate of death rate is between 0.1% - 0.2%.
3. Anyone who tests positive for COVID-19 and dies is labeled a COVID-19 death, so the death count is over estimated. The treating physician doesn't determine the cause of death.
4. Mandatory vaccination is offensive. If a vaccine is developed, it will be approved for use without long term safety testing.
5. Pharmaceutical companies have a track record of recklessly pushing dangerous drugs.
6. Be afraid of any tracking--RFID, phone apps.
7. Rant about Bill Gates not having medical training. He controls the WHO, which is setting US COVID-19 policy. He is using his non-profit foundation to gather power.
I’ll address claims out of order, because “YOU CANT TELL ME WHAT TO DO, I’M A REBEL!”.
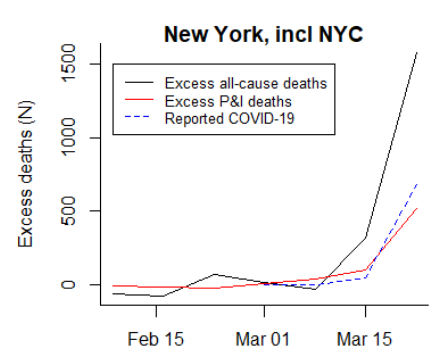
2. 26,000, or 1 in 700 (0.14%), of New Yorkers have already died of COVID-19, which provides a floor to estimates of the death rate. Estimates of incidence in New York range from 21% (New York city) to 3.6% upstate to 13% expectant mothers in New York, to 13.9% statewide incidence from antibody testing. Estimate that 20% of people in the state have had COVID-19, gives a death rate of 0.14% x 5 = 0.7%. But the confirmed death count is known to be an under count. The true death rate can be estimated by looking at how many people have died in NY this year and comparing it to a typical year. This gives an estimate that the COVID-19 mortality that is ~50% higher in NY than the confirmed death toll. So 0.7% x 2 = 1.4% mortality rate. A death rate of ~1% +/- 50% (0.5-1.5%) with good hospital care seems like a reasonable estimate.
In Iceland, testing a random sample of people gave an estimate that 2100 – 2800 people in the country had COVID-19, with 10 deaths, giving an estimated mortality rate of 0.36% – 0.48%.
So the incidence of COVID-19 is higher than reported with many people having mild disease. The US isn’t testing all symptomatic people, population surveys are only starting to report results.
Illinois reports 3,111 deaths and 70,873 cases, a death rate of 4.4%. But no one thinks that 4.4% is the death rate. A more reasonable estimate would be 50% more deaths, 4666 and 10X more cases, 710k, giving a mortality rate of 0.66%. The number of undiagnosed cases is where most of the uncertainty lies.
No one was reporting a mortality rate of 4.5%, that is bullshit. The early March results were all over the map, but no one took them seriously, they were early reports. And everyone knows the number of cases is higher, a lot of people with mild or asymptomatic disease, though there still is a lot of uncertainty as to how many people have had COVID-19.
It is still possible that the best estimates today are off, and that the mortality rate is lower. Let’s say it is 0.25%. Given that there is no vaccine, no one had any immunity to the virus a few months ago, and how easily it spreads, it would infect 2/3 of the country in a few months if it wasn’t slowed down. 2/3 of the US is 200 million people, 0.25% mortality would be 500,000 people. 2.5 million people would require hospitalization, but the US only has hospital beds for a small fraction of that number, so mortality rate under conditions of uncontrolled spread would be much higher.
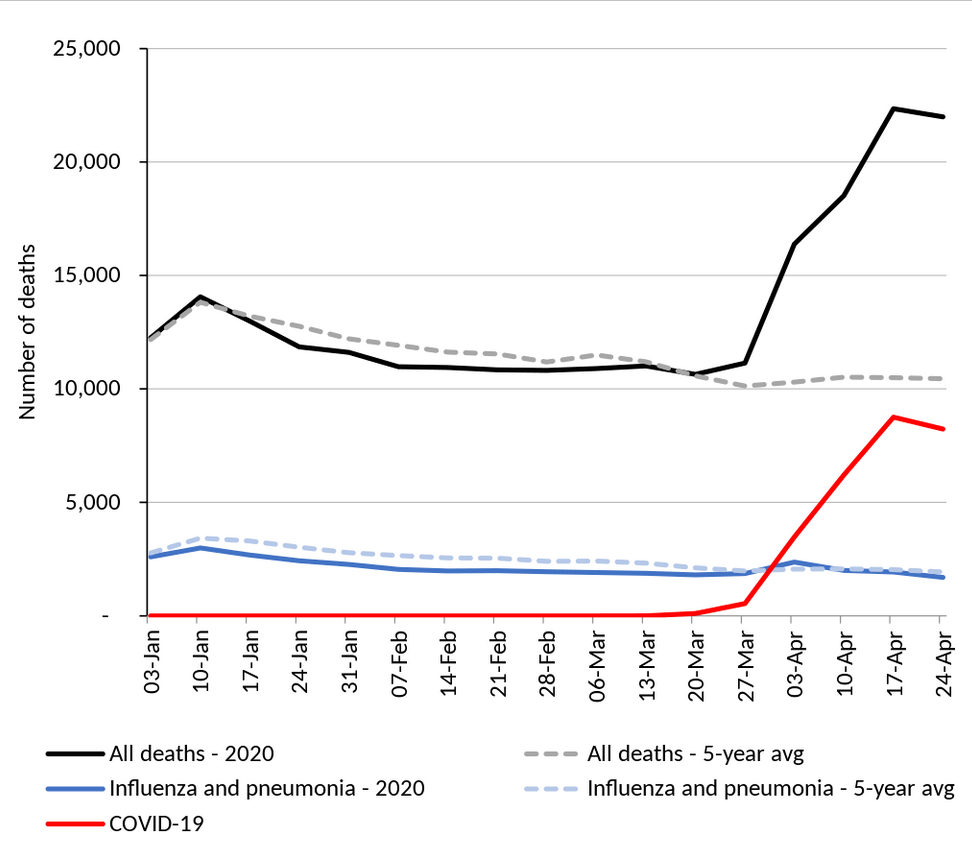
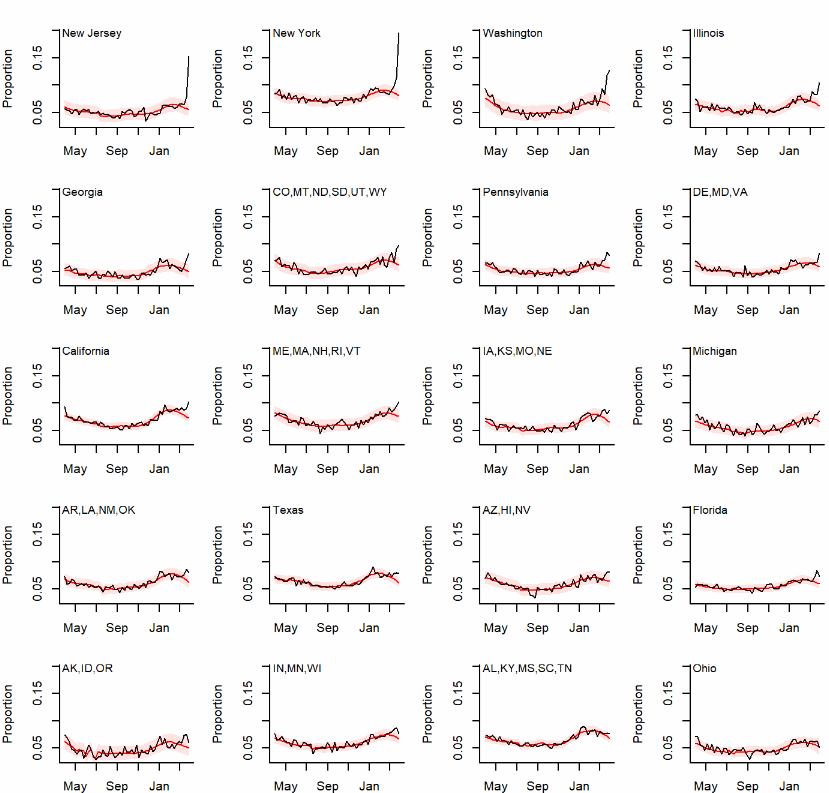
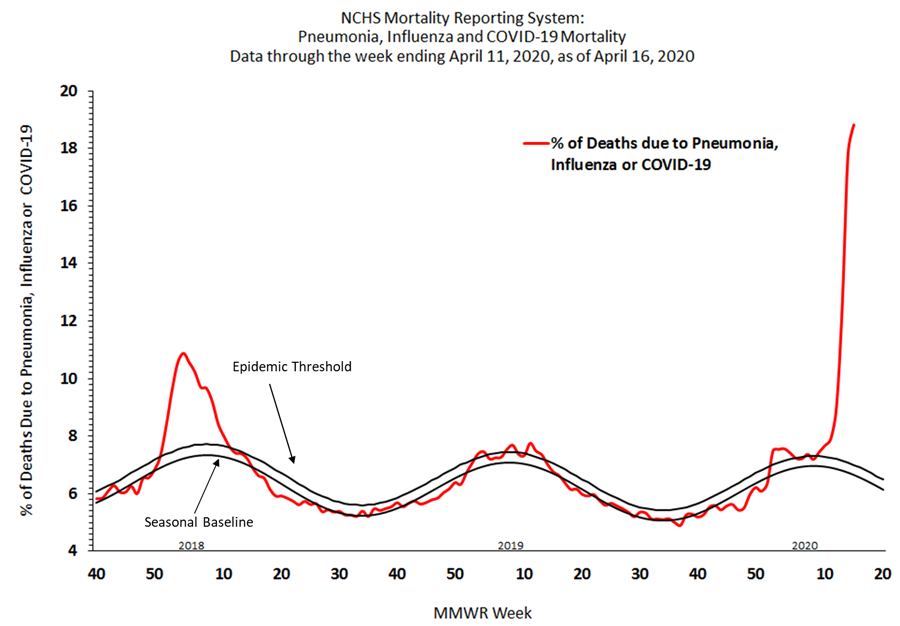
Here are graphs of excess mortality, NY, UK, US state estimates, and CDC (NCHS) reporting:
3. This is a conspiracy theory that grew out of an interview Minnesota State Sen. Scott Jensen, a family physician, did with Fox News host Laura Ingraham on April 8. This turned into a meme, “hospitals get an extra $13,000 if they diagnose a death as COVID-19!”. There is no evidence for this, and Jensen now says his statements were misconstrued.
COVID-19 deaths are being reported by doctors using the existing practices. That there are *lots* of COVID-19 deaths can be seen from the rise in overall mortality this year. The CDC estimates disease prevalence and mortality using multiple lines of evidence–death certificates, testing of hospital samples, etc. This is how the yearly flu mortality figures are assembled by the CDC. It takes 1-2 years for these estimates to get finalized.
4. It will be interesting to see whether this blows up if a vaccine is developed. I could see the anti-vax movement colliding with the ‘taking COVID-19 seriously is a Democratic attack on freedom’ being pushed already by the President.
If a vaccine is developed, every sensible person will go out of their way to get it. Middle aged people who get COVID-19 end up in the hospital 2-3% of the time. Who wants to risk that? Also, widespread vaccination would allow us to open up the country again without triggering a new wave of cases. Will vaccination be mandatory for school children, or for people visiting nursing home or attending concerts? Maybe.
If a vaccine is approved, it will have gone through safety and efficacy testing. It will most likely *not* have been tested as thoroughly as a typical vaccine, because this is a crisis, and every day of delay costs lives. And costs people billions in lost income.
6. Until a vaccine is available, the best way to control the spread of COVID-19 is testing and track & trace. Identify and quarantine infected people, and identify and quarantine people that came in contact with them. There have been proposals to use tech–a phone app, or phone location data, to help identify contacts. Other countries are already using this successfully.
The fear that this will be used in the US to set up a permanent regime tracking everyone’s whereabouts all the time for… some sort of bad purpose is crazy.
1., 5., 7. The idea that a person shouldn’t take drugs made by pharmaceutical companies because they are keeping you sick to sell you drugs is, again, nuts. Disease exists, and before effective treatments, people suffered and died. Before modern medicine, people got lots of fresh air and exercise, many people ‘exercised’ all day long, and ate ‘all natural foods’ from the local farms, and they still got sick and died. This point seems unrelated to the COVID-19 rant.
Bill Gates has spent the last ~20 years working on public service projects–education and infectious disease. Not much has come of the education projects, but his funding of infectious disease projects has been very productive and is well-regarded. He knows more about epidemiology than almost everyone without a PhD in the subject. He’s been reading this stuff for years, for ‘fun’. Why are we hearing from him? He knows a fair amount about it, and America loves CEOs and rich guys. The WHO is an organization that coordinates efforts of world governments to fight disease. Like all UN efforts, it has little power and runs on cooperation and donations by member countries.
The idea that you should do what you think is best for yourself and screw everyone else is a very American idea. When it comes to skydiving and shooting heroin, I’m all for it. But this is a case where the behavior spreads disease and puts everyone at risk. A good analogy is drunk driving. Freedom, but never responsibility! Public health measures like quarantine, banning large gatherings, and mask wearing reduce disease and save lives. These are measures taken to fight a disease endangering the country, temporary measures directly aimed at stopping the spread of disease. I think it is reasonable to enact and enforce public health guidelines.